




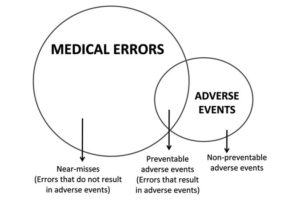
 As Ivan Illich pointed out in Medical Nemesis (1976), the reigning medical industry enjoys a virtual monopoly on defining “disease,” as well as on the endless production of lucratively patented new drugs ostensibly effective as treatments. “Public awareness” campaigns are highly selective: one situation is a world emergency, another is simply an ongoing “problem.” As to the latter, I am referring here to what are euphemistically designated as “preventable adverse events” (PAEs). This is used as a mortality-rate category: “medical errors” directly leading to the deaths of patients.
As Ivan Illich pointed out in Medical Nemesis (1976), the reigning medical industry enjoys a virtual monopoly on defining “disease,” as well as on the endless production of lucratively patented new drugs ostensibly effective as treatments. “Public awareness” campaigns are highly selective: one situation is a world emergency, another is simply an ongoing “problem.” As to the latter, I am referring here to what are euphemistically designated as “preventable adverse events” (PAEs). This is used as a mortality-rate category: “medical errors” directly leading to the deaths of patients.
In our current state of widespread alarm, we hear from medical authorities that this COVID pandemic could kill as many as 200,000 Americans. (We hear much less about the usually advanced age, as well as usual “co-morbidities,” of such persons — nor of the secondary (bacterial) pneumonia, hardly unusual in the hospital setting, which finishes so many of them off.) So a bit of skepticism, perhaps not too much, is still warranted in the current situation. How many elderly victims, in heavily polluted northern Italy, were also smokers? How many Chinese victims, in industrial (polluted) regions, were smokers? (Hint: almost half of Chinese men smoke, but smoking is becoming less prevalent in China.)
In such a rapidly growing crisis, the U.S. Congress comes to the rescue — with multi-trillion-dollar appropriations, much of it public-financed subsidy/investments in privately owned medical research initiatives (e.g., the usual “race for a vaccine”). Sound familiar? (Read: “corporate socialism — as in, “The “War” — on something hard to measure but nonetheless looming menacingly — “Terror.”) In that particular case, of course, the rapid result was the doubling of the Pentagon/”national security” budgets, as well as the creation of yet another federal department, “Homeland Security.”
But to return to those PAEs. Is it not a widespread medical emergency when such PAEs are directly causing up to 400,000 deaths in the U.S. every year?? ((John James, Ph.D., “A New Evidence Based Estimate of Patient Harms Associated with Hospital Care,” Journal of Patient Safety, September 2013.)) Another published study only estimates a (minimum) figure of 250,000 ((“Study Suggests Medical Errors Now Third Leading Cause of Death in U.S.” John Hopkins Medicine (report), May 3, 2016.)) — which still would make PAEs “the third leading cause of U.S. deaths annually.” Moreover, unlike epidemics, such deaths are, by definition, preventable — should hospitals invest sufficient budget in more safety-measures and correctives (as well as avoiding the cash-cow of largely unnecessary, and potentially complicated, coronary surgeries ((Nortin Hadler, M.D. Worried Sick: Overmedicated America (chapter 2), University of North Press, 2012.)) ). By the way, the PAE estimates reported in these studies generally do not include the hard-to-measure but nonetheless clearly tens-of-thousands of annual U.S. fatalities due to “used-as-directed” prescription-drugs (most lethally, such notorious “medications” as Vioxx and Oxycontin).
To sum up: using a crude estimate — after all, why be too precise when only millions of lives are being terminated? — one can reasonably suppose that as many as 500,000 Americans, per year, are being killed — due to such PAEs and unsafe drugs — by their profit-driven, cost-cutting “health care system.” Need I say more?